

Introduction: Large B-cell lymphoma (LBCL) is the most common subtype of non-Hodgkin lymphoma. Front line therapy is curative in about 60% of patients; however, about 30% of patients relapse and about 10% are refractory. For patients failing the front line, stem cell transplant (SCT) is currently the only curative option in second line of therapy (LOT2). This study examined real-world treatment patterns with curative intent in patients with relapsed or refractory LBCL to understand the unmet medical need in the United States.
Methods: This retrospective study used IBM MarketScan® Commercial and Medicare Supplemental Databases. Patients with ≥2 LBCL diagnoses on different days in 1/1/2012 - 3/31/2019 were identified (index date = date of the earliest LBCL diagnosis). Patients who were ≥18 years of age on the index date, had ≥1 claim for any LBCL treatment on or following the index date, ≥6 months of data prior to (baseline) and ≥12 months of data after (follow up period) the index date, and had no baseline LBCL diagnosis were included. Treatment patterns, including lines of therapy (LOT), treatment regimen, duration of LOT and time from the end of a previous LOT to the subsequent LOT, were examined. All patients were required to receive first LOT (LOT1) of R-CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone +/- rituximab), EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin hydrochloride +/- rituximab), or regimens with anthracycline. Of those, patients were further required to receive LOT2 with SCT-intended intensive therapy or platinum-based chemotherapy as recommended by the National Comprehensive Cancer Network (NCCN). Patients were intended for SCT if they received an SCT-intended LOT2 regimen or received SCT regardless of LOT2 regimen. SCT was identified from the LOT2 start date to the end of the study period. All analyses were stratified by whether a patient was intended for SCT and by receipt of SCT.
Results: A total of 3,443 patients with LBCL received an eligible front-line therapy (mean age 59.2 years, male 56.9%, length of follow up 2.5 years, National Cancer Institute (NCI) adapted Deyo-Charlson comorbidity index 0.83). Top comorbidities were other malignancy (63.3%), diabetes (23.3%), psychiatric disturbance (13.9%), and chronic pulmonary obstructive disease (13.2%).
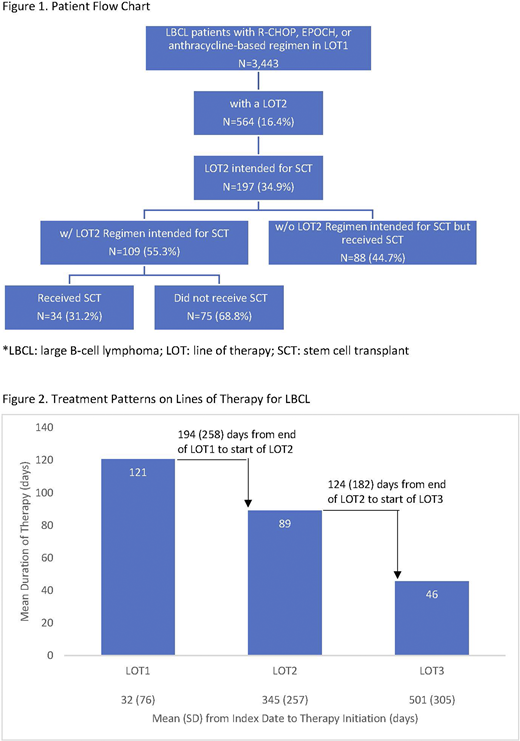
Among the LBCL patients, 564 (16.4%) received LOT2 with 197 (34.9%) patients SCT-intended and 367 (65.1%) not SCT-intended (Figure 1). SCT-intended patients were significantly younger than SCT-non-intended patients (55.9 vs. 60.9 years, p<0.001), and patients who received SCT were younger than those who did not receive SCT (53.6 vs. 59.7 years, p<0.001).
Among the 197 patients intended for SCT, only 55.3% (n=109/197) received NCCN recommended LOT2 for intensive therapy: ICE (ifosfamide, carboplatin, etoposide) +/- rituximab (32.5%) and GemOx (gemcitabine, oxaliplatin) +/- rituximab (19.3%) were the most common regimens. SCT-intended patients initiated LOT2 nearly one year (345 days) after and third line of therapy (LOT3) 501 days after their LBCL index diagnosis (Figure 2). Duration of LOT decreased as patients moved on to later LOTs (LOT1=121 [standard deviation (SD)=69], LOT2=89 [SD=145] and LOT3=46 [SD=23] days). Likewise, the time between 2 consecutive LOTs decreased (194 [SD=258] days between end of LOT1 and start of LOT2, 124 [SD=182] days between end of LOT2 and start of LOT3). Steroids were often prescribed during LOT1 (82.2%) and LOT2 (74.6%) as concomitant therapy. Among the 109 patients receiving SCT-intended regimens, only 34 (31.2%) went on to receive SCT. An additional 88 patients received SCT without being observed to receive an SCT-intended regimen. They might have received therapy in the inpatient setting, which could not be captured in claims data. Among the 82 patients with LOT3, 60.1% received SCT and 9.8% received Chimeric antigen receptor (CAR) T cell therapy.
Conclusion: The findings provide insight into real-world treatment patterns in patients with LBCL who received SCT-intended therapy. A small proportion of LBCL patients received NCCN recommended SCT-preparative regimens in LOT2 and only 31% of them received SCT. This highlights the magnitude of unmet need for relapsed or refractory LBCL patients. Future studies should examine the impact of new therapies on the management of LBCL.
Thornton Snider:Kite, A Gilead Company: Current Employment; Gilead Sciences: Current equity holder in publicly-traded company, Research Funding; Precision Medicine Group: Ended employment in the past 24 months, Research Funding. Cheng:Kite, A Gilead Company: Current Employment, Current equity holder in publicly-traded company. Song:IBM Watson Health: Research Funding. McMorrow:IBM Watson Health: Current Employment. Diakun:IBM Watson Health: Current Employment, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal